
“… with a rubber hose!” used to be a childish insult from my kindergarten years. What I’m considering putting up my nose is a dilute Betadine (povidone iodine) spray the next time that I get viral upper respiratory tract infection symptoms (runny nose, sinus congestion, cough, sore throat).

I don’t know how I had missed this recommendation during the Covid Era as a potential tool to help reduce nasopharyngeal viral load. I think I’d seen it mentioned some months back and had dismissed it without the slightest consideration. Now, with the Omicron variant that has been shown to primarily replicate in nasal epithelial cells, it stands to reason that delivering an easily tolerated virucidal agent directly to that region might be a very focused help.
I recently saw the nasal spray recommendation again (by Dr. McCullough) and have been looking into it as an option this morning. As I do a Duck Duck Go search (for less biased results), I find a number of pro and con stories.
There are the typical knee-jerk reflexes against anything that isn’t either vaccine or remdesivir for CV19 treatment. For the life of me, as a physician, it is difficult to understand the extreme and emotional vehemence against any of the inexpensive, low risk, early treatment therapies that might aid in reducing viral load or replication, symptoms, inflammation or thrombus formation. (That is a detailed tangent for another time.)
There are plenty of iodine naysayers, including a Rolling Stone article that provides the typical mocking disbelief of something the writers describe as anti-vaxx lunacy. What I know as an anesthesiologist, from a baseline of long established practice, is that perioperatively it is routine to use an iodine (or other antimicrobial) nasal swab treatment in order to reduce nasal pathogen colonization in an effort to minimize surgical site infections. So, the concept of nasal antimicrobial prevention and treatment is neither fringe nor without medical/scientific basis.
What I want to know, as every thinking adult should approach similar topics (and life, in general), is what are the proposed mechanisms, rationales, costs, risks and evidences of any purported intervention or claim – be it medical, political, economic or social. So, I’m looking it up and giving it thoughtful consideration rather than trusting the process of reason and deduction to the politicized and hysterical actors we find in today’s chaotic environment.
A review of the literature in 2020 by Frank, et al. in the Ear, Nose and Throat Journal found –
RESULTS: Povidone-iodine has been safely administered for up to 5 months in the nasal cavity and 6 months in the oral cavity. Concentrations less than 2.5% in vitro do not reduce ciliary beat frequency or cause pathological changes in ciliated nasal epithelium, upper respiratory, or mucosal cells. Adverse events with oral use have not been reported in conscious adults or children. Allergy and contact sensitivity is rare. Chronic mucosal use up to 5% has not been shown to result in clinical thyroid disease. PVP-I is rapidly virucidal and inactivates coronaviruses, including SARS-CoV and Middle East Respiratory Syndrome (MERS).
More recently, a Bangladeshi study (… I’m wondering if NIH and US Pharma are likely to fund such a non-lucrative investigation) by Choudhory, et al, and published in Bioresearch Communications in January 2021, randomized 600 patients to either saline or 1% iodine treatment and found the iodine group showed a negative PCR test much more quickly and was hospitalized at a much reduced rate. There was also no thyroid function disturbance from the iodine therapy, which has been listed as a concern by detractors.
Khan, et al., in the American Journal of Otolaryngology in Sept/Oct 2020 describe using dilute 0.5% povidone iodine as nasal drops and gargle for their study of over 300 patients prior to inpatient and outpatient procedures, as well as for exposed staff. This concentration is commonly used and tolerated in eye care, and was used without incidence. They note that iodine concentrations as low as 0.23% have resulted in zero viral activity after two minutes for SARS-CoV.
Dr. Mostafa Arefin published in April 2021 in the Indian Journal of Otolaryngology and Head Neck Surgery the clinical experience he and his 50 colleagues have had with their iodine protocol. Arefin, personally, has seen over 7,000 patients through the Covid era, performing hundreds of ENT procedures and surgeries. He recommends the nasal therapy as a safe, cheap, easy and effective adjunct for Covid therapy, or prevention when exposed.
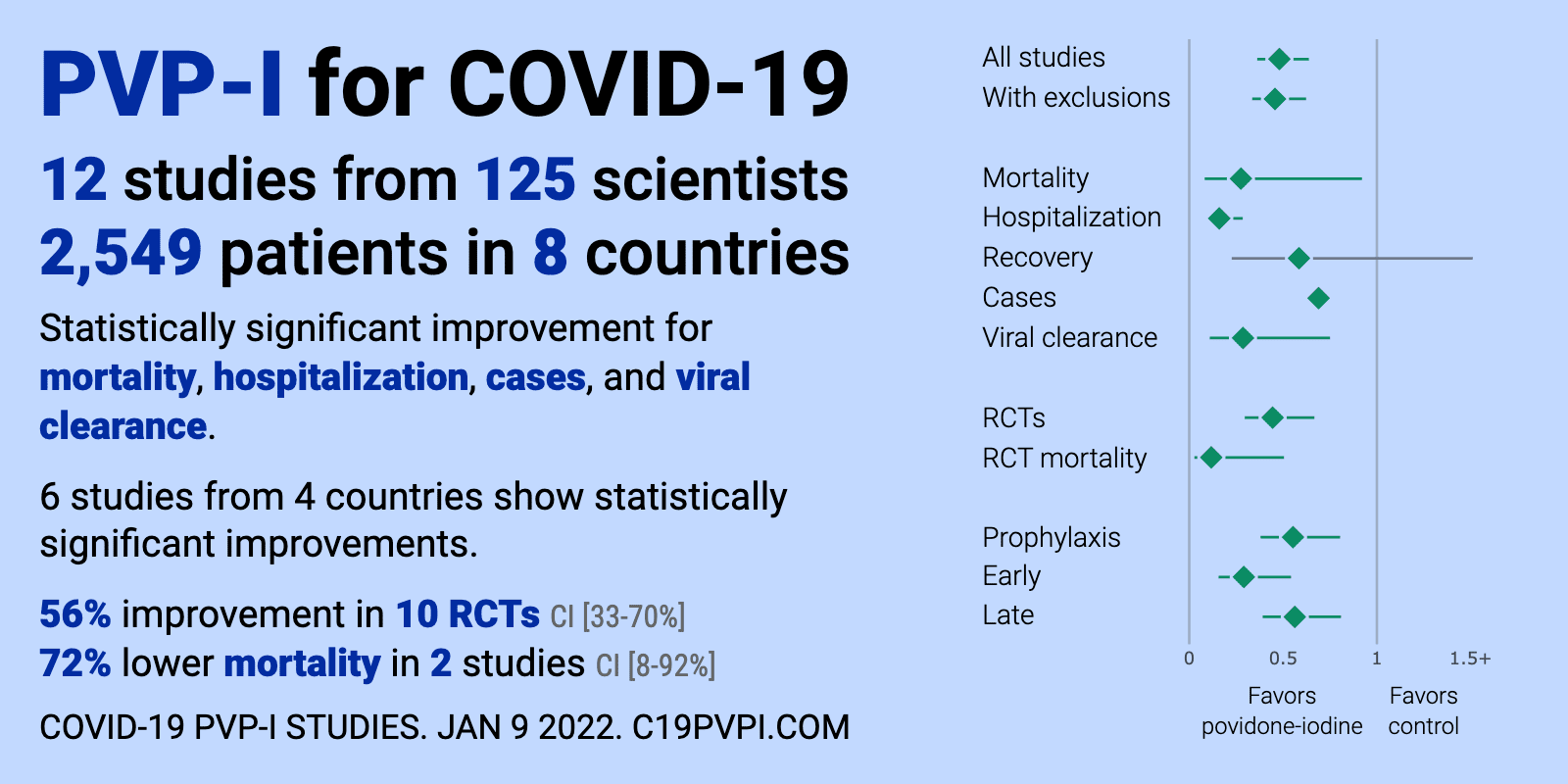
The physicians from Front Line COVID-19 Critical Care (FLCCC) Alliance have put together recommendations as Prevention & Treatment Protocols for COVID-19. Their povidone iodine literature review and database show clear benefit from early treatment, with improved outcomes of viral clearance, hospitalization and mortality.
{kind=link}
Interestingly, it is apparently a well-accepted Covid therapy in both U.S. and British dental practices to follow a nasal/oral iodine wash for both patients and staff. Challacombe, et al. describe this in a May 2020 letter to the editor of the British Dental Journal.
While I am not making a medical recommendation to anyone that they use nasal iodine spray, for myself, it certainly seems reasonable as an early treatment adjunct to potentially reduce viral load and replication, decrease transmission, shorten the course of the illness, and improve outcomes. The fact that the concept could be so energetically maligned and immediately rejected by mainstream actors is curious.
It took a little time this morning to investigate some of the arguments and evidences on this topic, but now I have made an informed opinion about a potential role for nasal iodine as an early treatment adjunct for Covid (and potentially for other respiratory infections), in combination with other appropriate therapies… which can all be similarly investigated on their merits, failures and medical/scientific grounds. With additional future information, I reserve the right to alter my opinion. While certainly not all-encompassing, I find this morning’s investigative approach far superior to unquestioningly following a tribal, politicized, emotionalized, divisive reactivity that creates sides and enemies over opinions of medical therapy (and so many other issues that are often misrepresented!).
Dr. Jesse Santiano has a site I just found in which he describes a number of different iodine concentrations, preparations and possible applicators. Generally speaking, if you want to make a dilute 0.5% nasal/oral rinse, then start with the typical bottle of 10% povidone iodine (Betadine) that can be found in any pharmacy aisle. Add 1 teaspoon of iodine to make a 1/4 cup of DISTILLED (not tap, which may carry more resistant pathogens) water – a 1 to 20 dilution.
Turn off the TV. Exercise great caution with the self-proclaimed experts and the typical information flows. Go look some stuff up for yourself. And if you find yourself getting angry at a person or topic, consider that you may be misled or misinformed. If you disagree with any of this, you can stick it up your nose! (Just kidding.)