If we look at the lockdowns as treatment of the virus, or at least as medical prevention, then part of that prescriptive responsibility is to know the side effects and costs of that treatment. The four principles of medical ethics must be considered: individual autonomy, justice, beneficence, and non-maleficence.
What autonomy is left to the individual via lockdown?
Are the lockdowns just?
Is there scientific evidence that the lockdowns are beneficial to patient (and society)?
Do the lockdowns cause harm to individual (or society)?
There are many doctors (most, I imagine) that unquestioningly conform to “lockdown as prevention” as prescribed by state and federal governments. I do not believe that the prescription meets ethical or scientific criteria. I’ve shared some of the scientific failings and costs through my previous posts and links to others’ articles and interviews, including those of other physicians and epidemiologists.
So, how then SHOULD we proceed in an effort to mitigate the viral threat? Certainly, steps can be taken which can have an effect without causing harm.
Ethically consistent: encourage social distancing while continuing much of life, work or study from home as able, allow anyone to isolate at home who so desires, protect the elderly and ill from outside contact as possible, encourage hygiene and general healthy living, offer broad testing to track spread and immunity trends, collect and share confirmed data (not guesses, and assumptions).
Unethical: mandates by coercion and threat of force that prohibit work, travel or association. Fines and arrests for violations. Shaming and intimidation tactics to discourage any challenge to mandates. Certainly, any private organization that desires to place a condition on its employees and patrons (wash hands, take temperatures, wear a mask, etc.) is free to do so, as those persons are free to associate or not with that entity.
COVID-19 lockdowns continue. Much of the country has been prohibited by federal and/or state governments from working, moving about, purchasing “non-essential” items, or associating freely (even with masks and distancing). Churchgoers and clergy for Easter services were fined or arrested in some areas. This is recognized as excessive precaution and government overreach by many, leading to protests in state capitols this past week.
Initially, back in early March and some weeks before, the fear was that hospitals would be overwhelmed and that there would not be enough ventilators and ICU beds to handle the critically ill and dying. That crisis scenario was how all of the economic and societal lockdown was promoted. That was the marketing for “flatten the curve.” With some exceptions in high density populations, especially New York City, hospitals are generally well under capacity, in economic crisis, furloughing staff (140 hospitals identified as of today, per Beckers Hospital Review). There ARE enough ventilators. Initial projections of deaths were up to TWO MILLION, then revised down to 250,000 with social distancing and quarantine models. We’re at 33,000 deaths in the U.S., as of 17 April 2020 (potentially inflated as no testing is required to add COVID as a “suspected or likely” cause to the death certificate per CDC guidelines). We are 2 orders of magnitude lower in deaths than the original estimates. That seems meaningful.
While there are hospitals in select areas (primarily the densely populated New York City metro area) that have been at capacity, the U. S. medical system has not been overwhelmed. While news reports provide shocking pictures of a few hospitals requiring corpse overflow for their morgues, military and national guard makeshift hospitals and ships have not supplied direct COVID care or patient overflow assistance in significant numbers. They have essentially gone under- or un-utilized.
Economically, the government-imposed lockdowns have led to record unemployment. We now see food bank lines reminiscent of the Great Depression’s bread lines. The response is costing trillions through stimulus, contentious bailouts and new federal debt. The economic distortions, the picking of winners and losers, the market manipulation, all will have unpredictable, and certainly undesirable outcomes in the cost column… with an uncertain benefit in regards to reduced viral transmission and death. These unintended consequences cannot be predicted. As 19th century economist Frederic Bastiat wrote about in The Law, there is “the seen and the unseen.” We see lockdowns, stimulus checks and government attempts to intervene into the economy. However, we cannot see what those downstream and long-term effects will be, or what might have been if one entity or set of persons were not artificially preferred over another. Which jobs and businesses would have survived? Which benefited corporation or bank perhaps should have been allowed to fail? Which individual choices and avenues will never become available to us as a result?
Continuing the point of view from my previous blogs here and here, I argue that the attempted cure for this strain of virus appears excessive for its level of risk and is likely to have greater cumulative negative effects on economy and society than the virus itself. The attempts to “flatten the curve” of the viral peak which could strain the medical system will cause a much larger, longer and higher peaked curve of societal damage. Admittedly, in the early days of CV-19, there was far too much unknown. Extreme caution can be excused, maybe even applauded, despite the decades of funding of government entities which should have been generally watchful and prepared for such events with appropriate plans and equipment, even if the pathogen was yet unknown. (CDC, FEMA, WHO, perhaps even the CIA for failed global threat analysis,… are they good for anything other than drone bombs, black site renditions and torture? Anyway…. ) The American taxpayer has certainly paid dearly for these entities and should expect appropriate pandemic plans and logistics to have been in place for early and brisk response. That’s an article for another time.
However, we now can see data and inputs which provide improved perspective… or those can who are not paralyzed by the fear, emotion and reflex defense of their initial responses, ideas and policies which they are resistant to dial back. As always, there are considerable political investments and exploitative gains at stake for just such useful crises, which create conflicting incentives for interventionism. Regardless, as reasoning, analytical human beings, we should use new information and conditions to adapt our response and planning.
It is time for low-risk Americans to cautiously get back to life. There is a middle ground between careless frolicking about during high virus season versusthe lockdown of all living things. In Taiwan, for example, children were kept out of school for a few weeks then returned with daily screening and increased sanitation measures. Citizens showing signs of illness were quarantined and their progress tracked. Social distancing was especially encouraged with the elderly and those with co-morbidities. People generally have been able to work, function and live while maintaining precautions. They have arguably done better at disease mitigation than any other country which has locked itself down.
For every life that it is argued could be saved through extreme lockdown conditions and government responses, what are the costs in quality of life, living, well-being, lost wealth, unfathomable national (and perhaps personal) debt and ongoing societal disruption? What will be the consequences of the interventions into lives and the economy over the coming months and years? How will the political powers and controls have expanded? How will the landscape for employment have shifted? Which businesses and jobs will not have survived? Who will have lost their employment-provided insurance? What will that effect be on the provision of medical care in the near and long-term? (And if this is the point where you say, “yeah, that’s why we need national health care”… I’m inclined to temper that thought with, “you do see what national health entities have failed to do in this one instance alone, right?” I’m not enthused to give them ALL of the health power. Again, an article for a different time.)
Yes, people are still dying from the COVID-19 virus. It is serious. Of the roughly 2.8 Million Americans that die from all causes in an average year, per CDC data, the number of deaths so far this year from the virus is at 33,000 and climbing. It deserves significant attention. However, referencing my opening paragraph, 33,000 is not 2 million. It is orders of magnitude in difference. Perspective must protect us from societal paralysis and economic destruction. Our approach must be adapted with new data to allow us a reasoned and prompt way back to living – for the 99.95% of those among us who will survive. I hope to be among them. If I am not, at least I will not have promoted a legacy of destruction to plague the generations that follow.
Pandemics, climate change, natural disasters, destruction of civilizations, government excesses and collapses, famine, oppression, war, slavery, greed and exploitation, the rise and fall of many empires,… and the human perseverance, development, markets and successes over the thousands of years that trend toward improved quality of life, better standards of living, recognition of individual rights, decreased human misery and poverty. There is nothing new over the millenia. Some of it is just done differently, and online.
Perspective. The lessons of history. Immutable human nature. Cause and effect. Choices and consequences.
Just completed the audiobook. Thank you, Mr. Frankopan.
Posted inUncategorized|Comments Off on The Silk Roads: A New History of the World – by Peter Frankopan
I wrote last week about the novel coronavirus strain that has the world paralyzed. Of particular note is the experience in Italy with their ICU beds filled to capacity. The state of that nation has driven increasingly drastic isolation responses in the US. As I’ve tried to get some perspective on Italy’s situation, I would point to a few tempering facts. 1) The rate of infection, the surge, or the “curve,” of cases is admittedly of concern for sudden capacity stress within the US hospital system. I just listened to a JAMA podcast (Journal of the American Medical Association) with a physician director of critical care in the hard hit Lombardy region of Italy. Around minute 9:00 he reports that their area has roughly 8 ICU beds per 100,000 population. In comparison, I found that the US may have 20-30+ ICU beds per 100,000. US capacity for care appears much better, by multiples. 2) Italy has an older population, with elderly and those with co-morbid states (cardiopulmonary disease and diabetes, for example) being primarily those who die from COVID. Per wikipedia search, Italy’s elderly are about 20% of their population, compared with 15% in the US. Of note, also, per prior wikipedia search, their smoking rate is 20% – higher than the US, although a smoking link with COVID mortality is assumed by me but not proven. So, there are some definite population differences. 3) To compare illness numbers, Italy in recent years has had influenza deaths averaging 17,000 per flu season. COVID deaths are numbered at 3,400. In addition, the World Health Organization COVID dashboard shows Italy’s new cases to be leveling off.
As China and South Korea seem to be mostly through their epidemic, deaths to date from COVID are 3,250 and 94, respectively (see WHO.int dashboard for those countries). In a bad year, influenza deaths worldwide can range between 250,000 and 650,000 (noted in previous blog). Again, admittedly, the surge of COVID may vastly outpace the rate of rise of influenza cases, as well as have a higher mortality rate. But as the data is collected the numbers do not look catastrophic. As testing of the population becomes more common, the mortality numbers are declining. Of course, much is still unknown, data is still being gathered, broader testing of the public is just being rolled out significantly this past week in the United States. However, we do have some data from the aforementioned and other countries, as well as cruise ship isolations/quarantines, that COVID is not the Spanish Flu of 1918 or the Bubonic Plague. From the public health, media and government responses, one might think it was and that disability and death were knocking on our doors.
Regardless of tempering data, this week has seen some (in my opinion) extremely authoritarian government mandates. US state governments have varied in their responses, but multiple states are in a condition of self-quarantine or in-home isolation for all citizens, work stoppage, forced closure of businesses. In my state of current residence, the Pennsylvania governor mandated closure of all non-life sustaining businesses. Some states have forbidden the gathering of more than 50 or 25 or even 10 persons… with calls to the public to report violators to the government. Restaurants that attempt to seat and serve diners have been shut down by law enforcement, with arrests made. Aside from any gross violations of Constitutional Law or the Bill of Rights which would guarantee citizens’ rights of speech, association, labor and movement, there has not been any appreciable civil libertarian resistance.
WHO.int COVID dashboard, as of 20 Mar 2020
Again, while COVID may carry higher infectious and mortality rates than influenza, examining numbers adds perspective. In the US, the current flu season has seen 36M confirmed cases, 370K hospitalizations and 22,000 deaths. In comparison, COVID here has caused about 15,000 confirmed cases and 200 deaths to date. This is no guarantee that the health care system could not become overwhelmed, but again, we’re seeing disease patterns and numbers here and elsewhere that permit insights and reasons for optimism, rather than panic and complete lock down.
Hospitals are preparing for potential surges of COVID related pneumonia cases. In order to make rooms and ICU beds available, as well as to minimize potential infectious spread, surgical cases are being minimized. My affiliate hospital in Pennsylvania stopped performing elective surgical and procedural cases (from OR to GI lab to interventional radiology). As an anesthesiologist who covers these sites and cases, I’ve observed our case load decrease by up to 75%. Another factor constraining our service is the national shortage of Personal Protective Equipment (PPE, like gloves, masks, goggles and disposable suits). Health care workers are uncertain of our exposure risk, especially from asymptomatic patients who may shed virus for up to 14 days. Universal precautions with typical surgical masks may not be enough as viral particles are aerosolized. A tighter fitting and more filtering mask, the N95 (used to protect against TB exposure), is in high demand and short supply, although companies are ramping up production.
Meanwhile, economic, social and governmental controls and fallout are increasing daily. I’ll post in the comment section some articles of interest as we proceed. While I do hope to persuade any readers to take a more tempered and thoughtful approach to this situation than what is being pushed by media and government, equally I write in order to create a log of an event that afterwards will likely quickly fade from memory, having been a precipitant to societal change which will certainly just be an accepted norm at some point in the near future, with historical perspective and roots retained by few.
from https://s.abcnews.com/images/Health/200312_wnt_covid_curve
COVID-19 hysteria is in full swing. In the interest of “flattening the curve” of peak cases that might stress hospitals with a rush of capacity-exceeding, ventilator-dependent patients, have we created a greater societal crisis with a much larger and wider peaked curve? In an attempt to avoid certain costs and strain in one aspect of the economy, have even greater ones been caused throughout many sectors of the economy and life, in general? Are all costs and benefits being considered? Do we have a broad and long enough perspective to temper the narrow public health focus?
Yesterday, apparently following the strictest recommendations of CDC guidelines, an affiliate hospital declared that any employee or physician that travels outside of THIS PART OF THE STATE will not be permitted back into the hospital for 14 days. There are staff members returning from vacation who will not be able to report to work on Monday. Staffing, call and vacation schedules are significantly disrupted. In this small realm, what are those losses and costs, both personal and financial? And what if the hospital does become stressed with increased patient loads, now with reduced staff?
In the US, store shelves are being emptied of toilet paper, water and foodstuff. Travel is restricted. Quarantines are in place. Sports at all levels, in general, are cancelled. The effects are everywhere: concerts, Disney World, airlines, schools, work places, basic human endeavors of everyday life. Is there an aspect of the economy that remains unaffected? There is massive financial market upheaval. Trillions of dollars are to be injected into the economy by the Fed to stave off a worsening crash. Bailouts for affected industries and small business are being discussed. A bill is before Congress to give everyone free virus testing, free medical leave, free family leave. What are these costs and consequences, and who will pay for it all? At baseline, the US government spends about a trillion dollars a year more than it takes in,… and has for multiple past presidential cycles. How is your 401K? How is your work affected? What are the effects on individual families, especially the poor? To be clear, a Coronavirus did not cause any of the events in this paragraph. This is all the result of the response to the virus, not its effects. We are still early in the viral cycle and the reactions to it. Subsequent costs and fallout will not be known for months.
Maybe the public health response is appropriate. I’m arguing that it’s excessive. We’ll never really know. Later, most people will just say, “if we hadn’t been aggressive in flattening the curve, more people would have died.” How do you prove a negative? The precedent has been set. True COVID incidence will never be known because testing cannot be performed appropriately now or in the near future. Therefore, true mortality rates cannot be accurately calculated. COVID may be a ubiquitous virus that is mostly unrecognized among the population, leaving only the most symptomatic to be tested, thus skewing mortality rates. Regardless, we have data from the World Health Organization dashboard that shows cases in China and South Korea to have peaked within a matter of weeks and then decline thereafter. Of those tested, the Chinese may have a mortality rate as high as 4%, and South Koreans of about 0.9%. A lesson may be that this is a self-limited illness for almost everyone and that population incidence peaks and declines relatively rapidly.
I’ll argue for caution, voluntary social distancing, good hygiene, prudent travel. I argue against controls, mandates, restrictions, quarantines. The politicians are scared and do not want to be blamed for failures to act. It is an election year, after all. They also tend to see every crisis as an opportunity to expand legislation, oversight, spending and the pleasing of their lobbies and voter base. As a counter balance to that force, healthy skepticism seems appropriate. As we saw 9/11 open wide the doors of state surveillance, COVID will set the precedent for physical controls on citizen movement,… if not a mild introduction to martial law and lockdown, as China and Italy have pursued recently.
What are you trading for the promise of health and safety? How much true risk is there to that health and safety for which you make these trades? Now that precedents are being set, where will the limits be placed? And how will it expand once accepted? What happens with the next bad flu season? Who gets the bailouts, the paid leaves, the quarantines, the closures? What will be voluntary, and what mandated? What are the penalties? Who are the enforcers? When does the National Guard get called in? At what Dow Jones Index level does the central bank take over the stock market? How are the infected tracked and surveilled? These are all issues of degree. To some, they may seem extreme questions, but we are far along that continuum of trades at this point.
Perhaps the country has purchased a small scale curve flattening, but in exchange created a large scale peak across the economic and political landscape of the United States. Tempering the response, and in some cases the hysteria and over-reaction, may help flatten the broader curve of societal damage and costs.
Posted inUncategorized|Comments Off on Flattening the Curve? Or Trading a Small Curve for a Very Large One?
I recently wrote about my new Type 1 Diabetes diagnosis, the quest for affordable meds and supplies, and the subsequent financial savings found through transparent pricing outside of my insurance plan. I summarized that health care “coverage” is very expensive, whereas medical services may be found much more affordably.
My next step was to
establish an ongoing primary care physician relationship. I contacted
one of the large medical groups that my insurance plan covers and
found that before meeting with the internal medicine physician, I
would be required to have two visits with a physician assistant
first. In regarding this option, I considered: (1) it is not
unreasonable for me to seek direct access to a physician rather than
being filtered through a physician extender, (2) especially in light
of a new and significant medical diagnosis, (3) it is reasonable to
anticipate having a personal relationship with my PCP, which would be
hampered if I can’t meet him or her for another 6 months or more, (4)
I am paying significant premiums for insurance “coverage” that I
expect to purchase me access to physician services, and (5) being a
physician myself, I want the expertise of a fully-trained,
board-certified specialist that exceeds my level of training in
general adult medicine. None of this is to denigrate our PA or NP
colleagues who are integral to the team approach of medical service
provision, but that is not the level of care that I choose to
purchase as my initial consultation. (I’m sure that some would
disagree with my opinion, but that topic is a debate for another
time.)
Having previously
visited a specialist in the above-mentioned medical group, I knew
that new-patient and follow-up visits would likely approximate the
specialist bills that I’d received: $285 and $127, respectively.
After insurance “adjustments,” my out-of-pocket co-payments had
been $166 and $87, respectively. Now, able to judge costs and service
level of that PCP option, I compared these to a Direct Primary Care
(DPC) practice that my daughter, Aubrey, had recently joined: Gentile
Family Direct Primary Care (pronounced Jin-TIL-ee), in
Pittsburgh, PA. I have keenly followed the DPC trend for several
years, but this would be my first foray into the field as a patient.
Dr. Natalie
Gentile’s initial fee is $100, followed by a $70/month membership
fee. Some of the benefits of joining her DPC practice include: same
or next day appointments of no less than 30-minutes duration;
unlimited office visits with her; direct phone, text and email
communication; and wholesale pricing for lab work, medications and
many diagnostic tests. I ran the numbers, then emailed her for an
appointment.
My first visit with
Dr. Gentile lasted an entire hour as she not only focused on my
medical issues, but on broader lifestyle, diet and family details.
She subsequently researched and emailed me options for wholesale
insulins and medical supplies. She saved me several hundred dollars
over average retail pharmacy pricing on medications that were not
covered by my insurance. Even had my insurance covered those meds,
the “discount” would not kick in until I met my $3,000
deductible.
Given my busy work
schedule during the week, I was not available to pick up my
medications and supplies during office hours, and did not want them
mailed to my home to sit on my front porch. Dr. Gentile stayed in
frequent email contact with me, and offered to meet me on a Sunday
afternoon so I could retrieve my meds! Needless to say, I have found
my Primary Care Home.
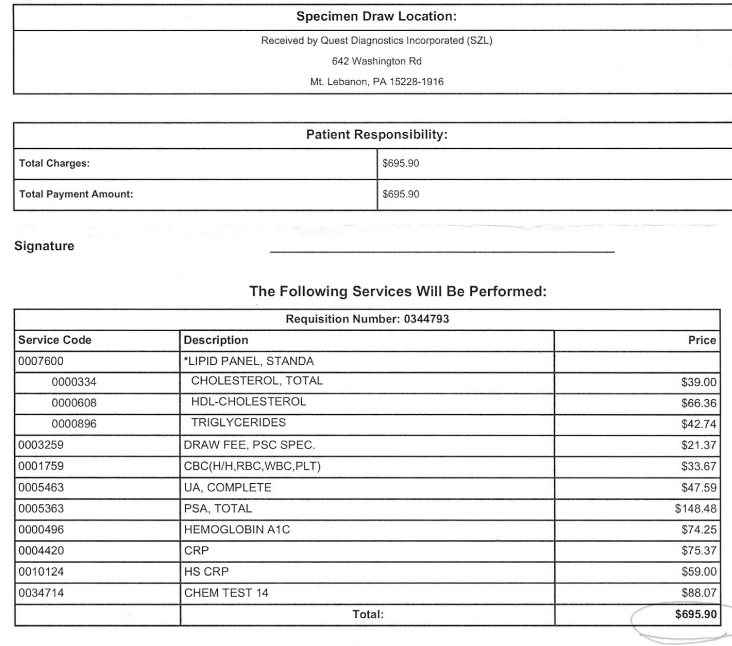
As I’ve promoted the idea of DPC, one of the concerns that I hear, and have had myself, is that the monthly membership fee might make the economics of the model unsustainable for patients. I calculated my own recent and projected medical expenses to get a comparison between insurance or retail pricing versus Dr. Gentile’s transparent wholesale pricing for visits and services. I project that in a year of quarterly “insured” PCP visits, I’d likely spend over $400 out-of-pocket, whereas with Dr. Gentile, I’ll spend over $900. However, comparing my recent lab work costs, I would have saved about $450 had she drawn the labs for me. Her wholesale prescription service will also save me at least $300 over a year compared to average retail prices. All told, I estimate a net savings of over $400 this year through my DPC membership. The potential for additional savings for other services is significant, particularly as I approach the age for screening colonoscopy – which she has coordinated for around $1,000 for her patients.
In summary, despite a monthly fee, DPC pays for itself (and then some) in many forms of savings and benefit. I believe DPC to be economically superior to the current third party payer model of medical practice. This is especially true for primary care and non-emergent outpatient medical services – which are arguably the majority of the demand in health care. I believe that DPC may be medically superior as this model allows physicians the time and flexibility to know their patients and accommodate their needs. DPC may also be superior from inter-personal, personal satisfaction, and humanistic aspects as the rushed, frustrating (for doctor and patient), insurance-restricted, 10-minute visit is replaced with greater availability, depth, flexibility, frequency and duration of interactions. Lastly, I consider the non-transparency of pricing in our profession to be a moral affront against the patient-consumer who has little idea of his financial obligation or exposure until after the fact. I can think of no other service or product line with similarly hidden and confusing costs. I have not found my own path to higher moral ground as a physician provider, yet, but I’m pushing us all towards greater awareness of costs and of systemic obstacles to transparency. For myself, as a patient, Direct Primary Care is a great stride forward.
Posted inUncategorized|Comments Off on My Path to Patient in a Direct Primary Care (DPC) Practice
I’m a healthy 48-year old anesthesiologist. At least I was healthy until an unintentional 20 pound weight loss over the summer, accompanied by unquenchable thirst, insatiable appetite, blurry vision, and the bathroom frequency of an elderly prostatic. My lab workup would reveal a high fasting blood sugar of 310 mg/dL, a very high hemoglobin A1C >14, positive urine ketones (showing that my body was breaking down muscle to use for energy), low levels of C-peptide (a byproduct of natural insulin production, revealing that my pancreas was making little insulin), and a glutamic acid decarboxylase (GAD-65) antibody level that was off the charts (which correlates with Type I diabetes due to autoimmune pancreatic islet cell destruction). So, today, I’m suddenly an insulin-dependent diabetic with a relatively rare case of Late Autoimmune Diabetes of the Adult (LADA). That will definitely alter your daily schedule,… as well as immediately put you in the market for a fair amount of pharmaceuticals and medical supplies.
Now
that I have my diet well-controlled with careful carbohydrate intake,
resulting in a relatively low insulin requirement, I’ve started to
look for ways to improve the diabetic lifestyle impediments that can
interfere with a busy O.R. schedule and active life. My initial daily
regimen has included four glucose checks a day (involving meters,
lancets, test strips, swabs, and cotton balls), and up to four
insulin injections: long-lasting NPH insulin twice daily as a base,
with a sliding scale of short-acting regular insulin at meals and
bedtime – all with syringes and vials. That’s a lot of stuff to
manage and carry.
from the Freestyle Libre website
I’m
transitioning to a single daily injection of ultra-long lasting
Triseba® (insulin degludec), supplemented with a once or twice daily
dose of Novolog® regular insulin as needed for fine-tuning: all by
easy-to-manage injection pens. The next step is to convert from all
the finger stick checks to a more streamlined glucose monitoring
system. After looking at the few continuous (and flash) monitoring
options out there, I’ve purchased the Freestyle
Libre® system. It consists of a small 14-day
subcutaneous sensor which attaches to your skin, transmitting your
glucose level to a hand-held scanner, or to an app on some cell
phones. That can save a lot of finger sticks, as well as reduce the
daily bulk and transport of required equipment.
The
savvy reader might have already questioned how much all of this stuff
costs. The short answer: it ain’t cheap. Goodrx.com
will show you that the most basic insulin vials of regular and NPH
can cost $150 each on the low end, with other types of insulin
running $300 to $1000 each per vial or pen. The other necessary basic
supplies can add $100 per month or more. Finding out the costs and
insurance coverages, formularies and deductibles, co-pays and
participating pharmacies is an exercise in frustration – and for
the patient reader, that’s where this article is headed.
When
I priced out the Freestyle Libre system with a recommended medical
supply company, applying my private insurance coverage with the
$3,000 deductible, the costs to me for Year One would have been:
Handheld reader – $300 each, one for work and one for home: $600
14-day sensor – $193 each x 26 (12-month supply): $5,018
So, of the $5,618 subtotal, insurance would pick up the
remaining $2,618 after my $3,000 deductible. I believe that my co-pay
for the sensors after the deductible was met was quoted around $70
each. That would leave me with another $900 or so for roughly
6-months worth of the “discounted” sensors.
That
all seemed a little pricey to me for a technology that cannot be more
complicated than my Android cell phone, Chromebook laptop, or
Playstation 4 – any of which cost me about the price of one single,
quoted glucose reader – in the neighborhood of $300. So, I started
looking for direct pricing. Goodrx.com
priced me readers and sensors for about $70 and $55 each,
respectively. That calculates to a Year One cost of roughly $1,600
– by paying out-of-pocket at Walgreens. Hmmmm… $1,600 versus
$5,600. For the exact same products. A FOUR THOUSAND DOLLAR
DIFFERENCE! A 350% markup, if my math is correct.
So,
it appears that I (coupled with my employer/group contribution) can
pay roughly $6,000 per year in insurance premiums for health care
“coverage,” then a $3,000 deductible before that coverage takes
effect, at which point I may still be liable for co-payments… and
then I get the privilege of being in the covered network for which I
will pay a markup of unnecessary, additional thousands of dollars. A
350% tax? Again, the savvy reader might question where all that money
goes, if just directly paying for a more transparently-priced medical
service or supply can be had so much more affordably?
The
thoughtful among us might also question:
What services are insurance corporations actually providing today?
Has the catastrophic medical insurance market morphed into an expensive, non-transparent, buyers’ club which surreptitiously raises prices for everyone while financially benefiting a potentially useless class of interlopers by skimming excess profits… perhaps to the tune of many billions of dollars per year?
What are the economic distortions in the medical market when true costs are difficult to acquire?
What is the cost of supporting the streams of third-party individuals, entities, organizations and bureaucracies that stand between a patient-consumer and a physician end-service, medical supply service or drug manufacturer?
What role is the FDA playing in encouraging or inhibiting competition, price transparency, and corporate protectionism?
What if you and your doctor have no idea what anything in the system really costs?
What if your doctor would happily provide you a service at a fraction of what your insurance “coverage” bills you?
What if your insurance company profits more in the health care transaction than does your physician?
What if she would be happy to charge you far less in a direct transaction… rather than participate in an awkward “provider-insurance corporation-subscriber” threesome of purposefully disjointed communication and secrecy?
What does it mean that in order to essentially avoid being defrauded of large sums of money, a patient like myself must spend many hours searching for solutions outside of the accepted “system” which enables that fraud?… And how much more difficult must it be for patients without health care experience to maneuver through that system?… Especially if sick and financially disadvantaged?
This
physician-patient, for one, has been awakened to the power of price
transparency and interloper-reduction. Health care “coverage” is,
admittedly, very expensive. In contrast, what do the actual medical
services and supplies cost, absent the interference and markup? What
if we could cut the price tag of our health care by 350% just by
pulling the costs out into the sunlight and eliminating the
unnecessary intermediaries in exchange for direct and transparent
care models?
Although
a minority of physicians and patients operate in a freer medical
market, there are well-established and growing options in play that
bypass opaque, expensive and unnecessary obstacles to affordable
medical services. Direct Primary Care (DPC)
practices like Atlas
MD and 1,000 others around the country;
transparently-priced surgery centers like Surgery
Center of Oklahoma and many others; advocacy
groups like the Free
Market Medical Association; Liberty
and other health shares; laboratory, radiology and pharmacy service
companies that offer transparent and discounted prices; and
comparison marketplaces like MediBid
to help you find them… all are growing service providers responding
to a demand for more transparent, understandable and affordable
medical services. By putting in a few hours of research as I did, you
may be able to save yourself thousands of dollars in unnecessary
medical costs. Few would deny that health care “coverage” is
expensive, but medical services do not have to be.
Posted inUncategorized|Comments Off on When Health Care “Coverage” Increases Costs
That’s how society thinks of Death… when it allows itself to think of Death… when a short exposure to someone’s serious illness or mortality temporarily intrudes into our consciousness. Death is something that happens to others,… or maybe to us, but in an extremely distant, unimaginable future. Meanwhile, in a false sense of immortality, in a state of willed forgetfulness and denial, we push those thoughts out of our minds. We distract ourselves with daily activities and pursuits that fill our lives with things, little pleasures, complicating and obstructive superfluous “necessities,” stuff, poorly-reasoned endeavors requiring high-energy and resources for the micromanagement of that which is potentially low value and difficult or impossible to control. Of that with which we fill our lives, how much just doesn’t matter? Or worse: harms, hinders, costs, indebts, dishonors us, causes regret?
By attempting to avoid reality, nature, and the ultimately inescapable life cycle, we may create for ourselves an erroneous perspective of our lives and of Life – a disorienting filter, or blinders, that mislead us down errant and poorly-reasoned paths. Our views of reality and our place in the universe become a self-deceptive lens through which we see with a skewed perspective, flawed vision, short-term sight. If what lies in the distance ahead of us cannot be imagined and mapped out, if we do not know even vaguely where we must go, how can we choose a path toward a meaningful destination?
How often do we travel a course in life without thought of where it will lead? What if we thoughtlessly (or purposefully) meander so far down a wayward road that there isn’t time left to correct our direction, to make amends, to create meaning and purpose? How often do we make decisions, large and small, with a limited vision, ignoring a longer term perspective, and without considering the consequences?
Recently, a friend gifted me a book on Native American perspectives – The Lakota Way – wherein Joseph M. Marshall, III, describes a seemingly much healthier view of Death with its rightful role in the life cycle of every living being. As such, it is the great equalizer which unifies us all – animal and man. Death comes for everyone, no matter how “powerful, famous, rich, beautiful, influential, irreverent, or lowly we are.” Death isn’t an enemy, but a friend and guide that “connects all living beings.” It is a “standard for truth against which all others are measured…. [N]othing can compare with its honesty and faithfulness.”
An awareness of our
mortality is a tool and guide to cut through noise, distractions, and
the appeal of short-term diversions at the expense of long-term
fulfilment. These insights reinforce to me that the acknowledgement
of our own impending deaths (hopefully distant and painless for us
all) provides a perspective that helps us to live well, to choose
well, to prioritize, to let go of the uncontrollable, to control only
ourselves, to de-clutter our lives, to treat others better, to
develop meaningful relationships, to stand for something, to create a
positive legacy, to leave this place better than we found it.
Of course, anticipating an impending death, some might say, “eat, drink and be merry, for tomorrow we die.” But this is a very short-term view in which one would attempt to avoid the consequences of his actions. For those that desire to live a long life, it is in their best interest to accumulate positive consequences, build long-term successes, minimize enemies and maximize friends, extend health, avoid waste and poverty, and experience joy over fleeting gratifications.
Although not a specific topic covered on this recent Tom Woods podcast, the mindset of mortality seems part of what was discussed by Tom with Michael Edelstein, PhD, in the episode “How to Conquer Self-Destructive Behavior.” Dr. Edelstein repeats throughout the conversation the distinction between our “needs” and our preferences. We tend to confuse the two, which can lead to poor decision making and misspent emotional energy – if not psychopathology. How often have we raised a personal preference to the level of absolute need, assigning it a false value and importance that causes us unnecessary anxiety, worry and perhaps fixation and torment.
Certainly, we need to eat, clothe and shelter ourselves, avoid physical pain, and deter a premature demise. However, we do not need to have a job that we enjoy, or to get along well with our boss. We may not want to lose a job, but we can typically find another. There may be a particular car, house, phone or shoe that we want, but the degree of importance and the level of acceptable expense that we may assign to that preference is not merited. What about the end of a relationship? Or a required move? Despite our strong personal preferences, what is needed to not only subsist but to thrive may be unrelated to our emotion-laden desires. What we often believe are needs, may merely be personal preferences created with a short-term perspective and infused with a high degree of emotional investment. Recognizing imperfect situations as inconvenient rather than catastrophic by employing a realistic and longer-term perspective, helps us make better decisions and prioritize our emotional energy. These views coincide with a mindset of mortality.
As I work on my own mindset of mortality, I hope to cut through the confusion and emotion of my own decision-making and priority-forming processes. I want to minimize my expenditure of energy, time and resources on what may not be of true significance or value. I want to be more self-aware, to create more meaning and purpose, to appreciate nature’s beauty and order, to sit quietly, to reduce consumption, to keep mindless distractions to a minimum, to foster ideas and ideals of justice and fairness and peace, to encourage and uplift and teach, to try to keep in perspective the daily frustrations and annoyances that are of minor importance, to let go more of what doesn’t matter – physically and emotionally, to recognize and better control my own emotions, to mindfully center myself more often, to foster positive relationships with those that I value, to create a legacy of which I can be proud, to leave the place better than I found it.
I invite you to join me in a mindset of mortality as we defy society’s avoidance of the topic. The denial of death, of our own mortality, is perhaps a sign of our personal and societal dysfunction – a divergence from nature, biology, reality, the universe,.. a psychopathology and self-delusion that impede healthy living, function and interaction. We’re all going to die. We’re all terminally ill from the moment of birth. Let us die well. In the meantime, let us live well in preparation for that eventuality.
Updated quote from a few years ago: “Please do not believe the slanderous accusations against me. I am not an anti-government extremist. I merely oppose those aspects of the government which coerce, steal, invade, surveil, threaten, kill, benefit and favor one group of individuals over another, misrepresent, defraud, reduce the individual to peasant status, grant special rights to persons with a government job or badge, mismanage resources and finances which lead to $21 TRILLION in debt, and practice war-based imperialism globally. On the other hand, I am in complete support of all governmental functions which promote the self-ownership, responsibility, independent thinking and function of the individual to pursue any life of choice which does not harm others. I just haven’t yet identified the existence of the latter.” – Todd Rice
Posted inUncategorized|Comments Off on Don’t believe the anti-government slander!
For most Americans,
the CIA is a secretive, but seemingly benign, agency of the
government that attempts to gather difficult-to-obtain information
for political or military use. The reality is that since WWII, the
Agency has been an uncontrolled clandestine and paramilitary arm of
government which operates with its own foreign policy objectives –
not infrequently in direct conflict with and purposeful opposition to
that of the President, military, Congress, and the will of the
American people.
Since its inception,
Presidents have rarely had an idea of the scope, violence, illegal
dealings (arms, drugs, bribes, coups), foreign government
interventions, foreign civilian deaths, subsequent global antipathy,
costs and absolute failures of the Central Intelligence Agency.
Congressional Intelligence Committees cannot break into the secrecy.
Often, Directors of the CIA, themselves, have been unaware of major
operations. Foreign branches and their directors often operate
independently, following their own arbitrary and personal agenda.
Author Tim Weiner,
is a New York Times reporter who has written on these topics for over
20 years, traveling abroad to pursue his stories where they take
place. With 170 pages of notes and references from an assortment of
documents, recordings, declassified materials, Congressional
testimony, interviews, etc., his best-selling book is well
documented. It serves as a rare glimpse into a dark and ugly space.
While intentions may
have been very good in the late 1940s and forward to protect the
American people, to fight the spread of communism during the Cold War
(which was in part an American creation by handing over Eastern
Europe to the Soviets at the end of WWII – a debate for another
time), and to have a global awareness of threats, the CIA became
something very different from an intelligence gathering agency. It
became a rogue agency without control or oversight, run by the whims
of Allen Dulles, his cronies, his minions, and their successors.
From innumerable
coups, to failed spy operations, to illegal financing schemes, to
arms/drug running rings, to whimsical murder and assassinations, to
the support of tyrannical dictators, to the unintended consequences
of the deaths of potentially hundreds of thousands of foreign
civilians, political prisons, black site torture centers, the
inception of war,…. What has taken place, often behind the scenes
and completely unbeknownst to you, has not been intelligence
gathering by the CIA, but rather the destruction of your security,
foreign disruption and death, the elevation of global anger and
resentment against the USA, the creation of terrorists, instability
and destabilization of societies around the world.
Legacy of Ashes is
an eye-opening opportunity to understand what certain aspects of your
government do to harm you, under false pretenses, with your tax
dollar, and without your consent. Instead of providing good
intelligence, more often than not, the CIA intelligence reports and
predictions have been 180 degree misreads of global events. The basic
story of the CIA over the past 70 years has been one of “comic book
fiaso,” as the author describes the Iran/Contra debacle. Of course,
there must be some good that the agency has done. Whatever that might
be, the seemingly endless list of harms and costs cannot justify its
existence.
Posted inUncategorized|Comments Off on Legacy of Ashes: The History of the CIA, by Tim Weiner



















{kind=link}