
COVID-19 lockdowns continue. Much of the country has been prohibited by federal and/or state governments from working, moving about, purchasing “non-essential” items, or associating freely (even with masks and distancing). Churchgoers and clergy for Easter services were fined or arrested in some areas. This is recognized as excessive precaution and government overreach by many, leading to protests in state capitols this past week.
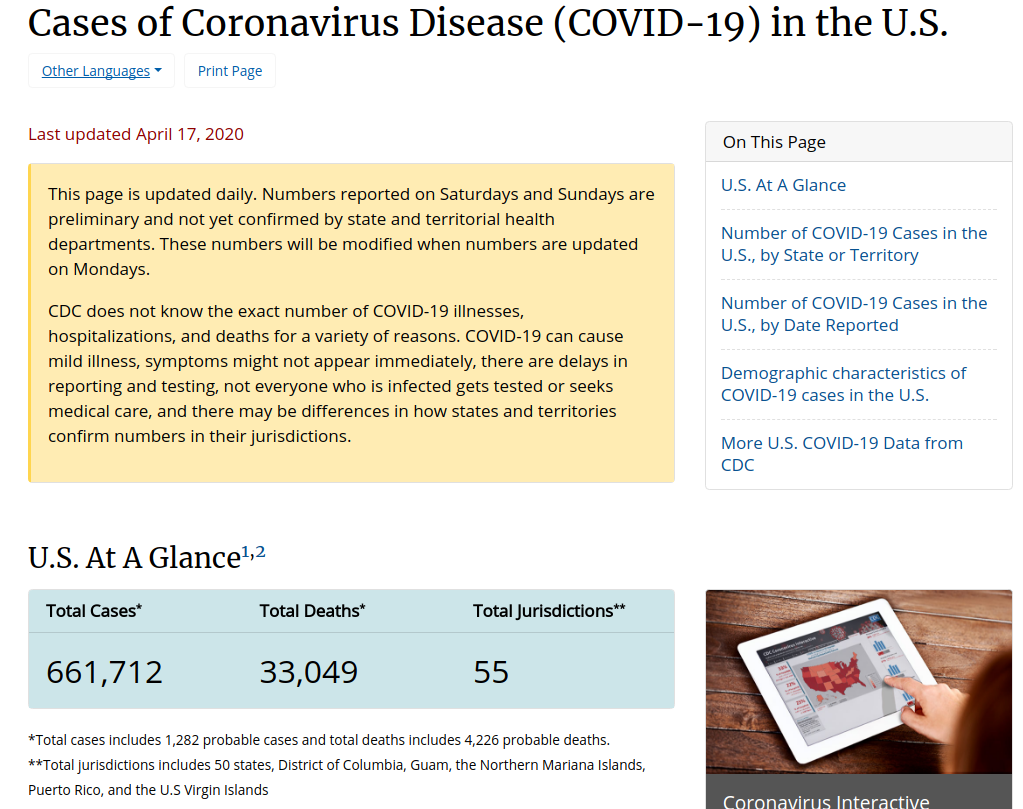
Initially, back in early March and some weeks before, the fear was that hospitals would be overwhelmed and that there would not be enough ventilators and ICU beds to handle the critically ill and dying. That crisis scenario was how all of the economic and societal lockdown was promoted. That was the marketing for “flatten the curve.” With some exceptions in high density populations, especially New York City, hospitals are generally well under capacity, in economic crisis, furloughing staff (140 hospitals identified as of today, per Beckers Hospital Review). There ARE enough ventilators. Initial projections of deaths were up to TWO MILLION, then revised down to 250,000 with social distancing and quarantine models. We’re at 33,000 deaths in the U.S., as of 17 April 2020 (potentially inflated as no testing is required to add COVID as a “suspected or likely” cause to the death certificate per CDC guidelines). We are 2 orders of magnitude lower in deaths than the original estimates. That seems meaningful.
While there are hospitals in select areas (primarily the densely populated New York City metro area) that have been at capacity, the U. S. medical system has not been overwhelmed. While news reports provide shocking pictures of a few hospitals requiring corpse overflow for their morgues, military and national guard makeshift hospitals and ships have not supplied direct COVID care or patient overflow assistance in significant numbers. They have essentially gone under- or un-utilized.

Economically, the government-imposed lockdowns have led to record unemployment. We now see food bank lines reminiscent of the Great Depression’s bread lines. The response is costing trillions through stimulus, contentious bailouts and new federal debt. The economic distortions, the picking of winners and losers, the market manipulation, all will have unpredictable, and certainly undesirable outcomes in the cost column… with an uncertain benefit in regards to reduced viral transmission and death. These unintended consequences cannot be predicted. As 19th century economist Frederic Bastiat wrote about in The Law, there is “the seen and the unseen.” We see lockdowns, stimulus checks and government attempts to intervene into the economy. However, we cannot see what those downstream and long-term effects will be, or what might have been if one entity or set of persons were not artificially preferred over another. Which jobs and businesses would have survived? Which benefited corporation or bank perhaps should have been allowed to fail? Which individual choices and avenues will never become available to us as a result?
Continuing the point of view from my previous blogs here and here, I argue that the attempted cure for this strain of virus appears excessive for its level of risk and is likely to have greater cumulative negative effects on economy and society than the virus itself. The attempts to “flatten the curve” of the viral peak which could strain the medical system will cause a much larger, longer and higher peaked curve of societal damage. Admittedly, in the early days of CV-19, there was far too much unknown. Extreme caution can be excused, maybe even applauded, despite the decades of funding of government entities which should have been generally watchful and prepared for such events with appropriate plans and equipment, even if the pathogen was yet unknown. (CDC, FEMA, WHO, perhaps even the CIA for failed global threat analysis,… are they good for anything other than drone bombs, black site renditions and torture? Anyway…. ) The American taxpayer has certainly paid dearly for these entities and should expect appropriate pandemic plans and logistics to have been in place for early and brisk response. That’s an article for another time.
However, we now can see data and inputs which provide improved perspective… or those can who are not paralyzed by the fear, emotion and reflex defense of their initial responses, ideas and policies which they are resistant to dial back. As always, there are considerable political investments and exploitative gains at stake for just such useful crises, which create conflicting incentives for interventionism. Regardless, as reasoning, analytical human beings, we should use new information and conditions to adapt our response and planning.

It is time for low-risk Americans to cautiously get back to life. There is a middle ground between careless frolicking about during high virus season versus the lockdown of all living things. In Taiwan, for example, children were kept out of school for a few weeks then returned with daily screening and increased sanitation measures. Citizens showing signs of illness were quarantined and their progress tracked. Social distancing was especially encouraged with the elderly and those with co-morbidities. People generally have been able to work, function and live while maintaining precautions. They have arguably done better at disease mitigation than any other country which has locked itself down.
For every life that it is argued could be saved through extreme lockdown conditions and government responses, what are the costs in quality of life, living, well-being, lost wealth, unfathomable national (and perhaps personal) debt and ongoing societal disruption? What will be the consequences of the interventions into lives and the economy over the coming months and years? How will the political powers and controls have expanded? How will the landscape for employment have shifted? Which businesses and jobs will not have survived? Who will have lost their employment-provided insurance? What will that effect be on the provision of medical care in the near and long-term? (And if this is the point where you say, “yeah, that’s why we need national health care”… I’m inclined to temper that thought with, “you do see what national health entities have failed to do in this one instance alone, right?” I’m not enthused to give them ALL of the health power. Again, an article for a different time.)
Yes, people are still dying from the COVID-19 virus. It is serious. Of the roughly 2.8 Million Americans that die from all causes in an average year, per CDC data, the number of deaths so far this year from the virus is at 33,000 and climbing. It deserves significant attention. However, referencing my opening paragraph, 33,000 is not 2 million. It is orders of magnitude in difference. Perspective must protect us from societal paralysis and economic destruction. Our approach must be adapted with new data to allow us a reasoned and prompt way back to living – for the 99.95% of those among us who will survive. I hope to be among them. If I am not, at least I will not have promoted a legacy of destruction to plague the generations that follow.
“Unfortunately, the media have tended to reinforce the initial ideas about what this disease was like which have not necessarily been borne out by the numbers since then.” – Dr John A. Lee, pathologist, NHS.
https://www.spiked-online.com/2020/04/17/theres-no-direct-evidence-that-the-lockdowns-are-working/
“Why lockdowns are the wrong policy” – Swedish epidemiologist and consultant to EU and WHO, Dr Johan Giesecke, explains Sweden’s more reasoned approach: socially isolate the elderly and ill, encourage adults to work and study from home without police enforcement, *hygiene*, kids still go to school, people can shop, people practice distancing, groups under 50 in number are permitted. He says the models have been unreliable and based on highly variable guesses, that the draconian lockdowns have no scientific basis, that governments have no viable criteria from which to back down from the lockdowns because there is no achievable goal (when deaths are zero for a month?), that this will likely be on the order of a severe flu season, that many millions of people have already had the virus and mostly been low to asymptomatic, that although typically the virus will take months of life from the elderly and ill it is the living that will deal with the aftermath of societal disruption and government excesses (especially the dictatorial trends of Eastern Europe), that even if lockdowns have an effect at slowing spread that ultimately the final death count will be relatively unchanged, no matter what you do this virus is a tsunami that will roll across the globe, fear and political gain drive the response rather than science, a major epidemiologic difference in COVID transmission and influenza is that the latter is driven by children whereas the the former is uncommon to affect the younger population,….
https://www.youtube.com/watch?v=bfN2JWifLCY
Another thought:
If we look at the lockdowns as treatment of the virus, or at least as medical prevention, then part of that prescriptive responsibility is to know the side effects and costs of that treatment. The four premises of medical ethics must be considered: individual autonomy, justice, beneficence, and non-maleficence.
What autonomy is left to the individual via lockdown?
Are the lockdowns just?
Is there scientific evidence that the lockdowns are beneficial to patient and society?
Do the lockdowns cause harm to individual, or society?
There are many doctors out there that unquestioningly conform to “lockdown as prevention.” I do not believe the prescription meets ethical or scientific criteria.
Ethically consistent: encourage social distancing while continuing much of life, work or study from home as able, allow anyone to isolate at home who so desires, protect the elderly and ill from outside contact as possible, encourage hygiene and general healthy living, offer broad testing, collect and share confirmed data (not guesses, and assumptions),…
Unethical: mandates by coercion and threat of force that prohibit work, travel or association. Fines and arrests for violations. Shaming and intimidation tactics to discourage any challenge to mandates. Certainly, any private organization that desires to place a condition on its employees and patrons (wash hands, take temperature, wear a mask) is free to do so, as those persons are free to associate or not with that entity.
“U.S. ducks coronavirus doomsday as projections miss mark”
Even in NYC, peak ventilator use was around 5,000. It’s shipping hundreds of ventilators elsewhere. Initial US deaths were modeled above 2 Million! Revised down to about 70,000 now. 2017 CDC data for flu and related pneumonia deaths was 55,000. So, for all of the shaming and ridicule of those that have said this could be similar to a severe flu season….
https://m.washingtontimes.com/news/2020/apr/16/us-coronavirus-projections-miss-mark-country-ducks/